ECG-SUMMARY-1
1. The ECG is recorded in a graph paper which is composed of small squares with 1mm height and width. Also 5 small squires form large squires in height and width. The X-axis represents Time and the Y-axis represents electric conduction. Every small squires 1mV in height.
2. Normally the ECG machine is set up to move the graph paper 25 mm per sec in the printer. Some times this may be changed up to 50 m.m/sec.
3. Each 1mm height in the Y-axis represents 1mV.
4. A normal ECG is composed of 5 waves namely P, Q, R, S, and out of which three waves namely P, R, and T are positive upward deflections and Q and S waves are negative downward deflections.
5. The waves are identified as follows. In a normal ECG the first positive upward deflection is known as P-wave. The P-wave represents the atrial (upper chambers)contractions.
6. The P-wave is followed by a QRS complex with an interval.
7. The QRS complex is the representation of the ventricular (lower chambers) contractions.
8. In the QRS complex the first negatively downward deflection immediately followed by R-wave is known as q-wave or Q-wave according to its size. In other words a Q or q-wave is any wave which is after the P-wave deflected downward immediately before the R-wave. The Q wave represents the brief repolarization of the Inter Ventricular Septum(IVS) when a brief and weak electrical conduction is passing from left to right across the (IVS). See Fig-1 below.
9. After the Q-wave within the QRS-complex any immediately following positive deflection is the R-wave or r-wave according to its sizes. In other words any upward deflections immediately followed by S-wave are known as R-wave. The R-wave represents a strong ventricular contraction due to strong conduction of electricity from right to left from the Purkinje fibers, the bundle of His and across the IVS(see Fig-1)
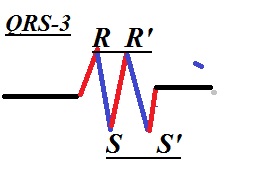
10. Then within the QRS complex a brief negative deflection immediately following the R-wave is known as the S or s wave as per its sizes. In other words any negatively downward deflection within the QRS-complex preceded by R-wave is known as S or s wave. see Fig-2 below.
3. Each 1mm height in the Y-axis represents 1mV.
4. A normal ECG is composed of 5 waves namely P, Q, R, S, and out of which three waves namely P, R, and T are positive upward deflections and Q and S waves are negative downward deflections.
5. The waves are identified as follows. In a normal ECG the first positive upward deflection is known as P-wave. The P-wave represents the atrial (upper chambers)contractions.
6. The P-wave is followed by a QRS complex with an interval.
7. The QRS complex is the representation of the ventricular (lower chambers) contractions.
8. In the QRS complex the first negatively downward deflection immediately followed by R-wave is known as q-wave or Q-wave according to its size. In other words a Q or q-wave is any wave which is after the P-wave deflected downward immediately before the R-wave. The Q wave represents the brief repolarization of the Inter Ventricular Septum(IVS) when a brief and weak electrical conduction is passing from left to right across the (IVS). See Fig-1 below.
 |
| Fig-1 |
9. After the Q-wave within the QRS-complex any immediately following positive deflection is the R-wave or r-wave according to its sizes. In other words any upward deflections immediately followed by S-wave are known as R-wave. The R-wave represents a strong ventricular contraction due to strong conduction of electricity from right to left from the Purkinje fibers, the bundle of His and across the IVS(see Fig-1)
10. Then within the QRS complex a brief negative deflection immediately following the R-wave is known as the S or s wave as per its sizes. In other words any negatively downward deflection within the QRS-complex preceded by R-wave is known as S or s wave. see Fig-2 below.
 |
| Fig-2 |
11.After the S-wave finally the ventricles relax after a brief interval which is represented by the S-T-interval.The T-wave is the final point or completion of one normal Sinus Rhythm. The next Sinus Rhythm starts again with the next P-wave. Hence the T-P interval, the interval between two Sinus Rhythms is the real isoelectric line as this line represents zero electric conduction in any situation whereas other wave intervals may deviate from the isoelectric line in abnormal conditions. (see Fig-3)
12. There are 12 leads that view the heart from 12 different angles. Out of which the bipolar electrode lead II is the hero which views the heart from the left bottom ankle which is more or less falls within the normal axis of the heart's electrical activities which is at -30 degrees to + 90 degrees. See Fig-4 below.
In the above figure note down the limb lead, II is viewing the heart from the bottom left which is more or less in the same ankle of the normal heart axis colored yellow in the circle. Hence the ECG recorded by this lead describes 80% of the total ECG representation.
aVR lead which views the heart from the extreme right gives the least representation of the total ECG.
Any ECG can be easily read out by looking at the lead II recordings which are at the bottom of your ECG report.
Lead aVL, I, are viewing the heart from the left anterior side
Chest leads V1, V2 looks the heart mostly the right Ventricular.
Chest leads V3 and V4, are looking at the left ventricle.
V5, V6, and aVL are viewing the heart from the left lateral side.
13.If in an ECG if there are negative deflections recorded by the left leads and positive deflections at the right leads indicates that there are abnormalities in your heart.
14. It is the theory of electrocardiology that if current flows towards the lead then it is recorded as a positive upward deflection in the ECG by that lead and vice versa. It is explained in Fig-5 above.
15. Axis is very important. Already we know that the axis of the heart is normally towards the downward left, southeast at an angle of 0 degrees to +90 degree. This can be seen in the ECG as +ve deflections in aVF, lead I, and II.
More commonly the normal axis is extended beyond 0 degrees up to -30 degrees from +90 degrees. This can be seen in the ECG as positive deflections in aVL, lead I and II, and negative deflection at aVF.This is shown in the following diagram. (Fig 6A)
There are three types of the deviated axis which we can observe easily in the ECG. The three deviations are illustrated in the following figure (Fig-6B)
In the above Fig 6B the 3rd diagram shows the presence of Left Axis Deviation (LAD). This can be observed in the ECG as follows:
The electrode aVL and lead-I show positive deflections and all others show negative deflections. This condition indicates that there is left ventricle enlargement and right ventricle's weakness. Also due to the left anterior fascicular block.
The 4th diagram shows the presence of Right Axis Deviation (RAD). This can be observed in the ECG as follows:-
Only electrode aVF and lead-III show positive deflections and all others show negative deflections. This condition indicates that there are a right ventricular enlargement and a weak left ventricle. Also this may be due to the right anterior fascicular block.
The 5th diagram shows the presence of Extreme Deviation which is a rare but dangerous condition. This can be observed in the ECG as follows:-
Only aVR electrode shows positive deflections. This indicates
atrioventricular canal defects. Also this may be due to extreme and heavy enlargement of the right ventricle and light and weak left ventricle. There may be a right anterior and posterior fascicular block or ventricular tachycardia.
16. Fundamentally we should keep in our mind that the augmented electrodes and the limb leads are looking the heart in vertical views and the pericardial or chest leads looks the heart in close horizontal views and concentrated towards the ventricles.
V1and V2 view the right ventricles, V3 and V4 view the interseptum and to some extend overall view, and V5 and V6 view the left ventricle. See the diagram below.
 |
| Fig-3 |
 |
| Fig-4 |
In the above figure note down the limb lead, II is viewing the heart from the bottom left which is more or less in the same ankle of the normal heart axis colored yellow in the circle. Hence the ECG recorded by this lead describes 80% of the total ECG representation.
aVR lead which views the heart from the extreme right gives the least representation of the total ECG.
Any ECG can be easily read out by looking at the lead II recordings which are at the bottom of your ECG report.
Lead aVL, I, are viewing the heart from the left anterior side
Chest leads V1, V2 looks the heart mostly the right Ventricular.
Chest leads V3 and V4, are looking at the left ventricle.
V5, V6, and aVL are viewing the heart from the left lateral side.
13.If in an ECG if there are negative deflections recorded by the left leads and positive deflections at the right leads indicates that there are abnormalities in your heart.
 |
| Fig-5 |
More commonly the normal axis is extended beyond 0 degrees up to -30 degrees from +90 degrees. This can be seen in the ECG as positive deflections in aVL, lead I and II, and negative deflection at aVF.This is shown in the following diagram. (Fig 6A)
 |
| Fig-6A |
There are three types of the deviated axis which we can observe easily in the ECG. The three deviations are illustrated in the following figure (Fig-6B)
 |
| Fig-6B |
The electrode aVL and lead-I show positive deflections and all others show negative deflections. This condition indicates that there is left ventricle enlargement and right ventricle's weakness. Also due to the left anterior fascicular block.
The 4th diagram shows the presence of Right Axis Deviation (RAD). This can be observed in the ECG as follows:-
Only electrode aVF and lead-III show positive deflections and all others show negative deflections. This condition indicates that there are a right ventricular enlargement and a weak left ventricle. Also this may be due to the right anterior fascicular block.
The 5th diagram shows the presence of Extreme Deviation which is a rare but dangerous condition. This can be observed in the ECG as follows:-
Only aVR electrode shows positive deflections. This indicates
atrioventricular canal defects. Also this may be due to extreme and heavy enlargement of the right ventricle and light and weak left ventricle. There may be a right anterior and posterior fascicular block or ventricular tachycardia.
16. Fundamentally we should keep in our mind that the augmented electrodes and the limb leads are looking the heart in vertical views and the pericardial or chest leads looks the heart in close horizontal views and concentrated towards the ventricles.
V1and V2 view the right ventricles, V3 and V4 view the interseptum and to some extend overall view, and V5 and V6 view the left ventricle. See the diagram below.
 |
| Fig-7 |
In Fig 7 the location of the chest leads is shown diagrammatically. From the position of the chest leads we can observe any problems in the ECG.
Any problem in the right ventricle the V1 and V2 record negative deflections.-
Any problem in the left ventricle can be clearly notified at the V5 and V6 deflections.
Continued.....