MYOCARDIAL INFARCTION-HEART ATTACK
We have already seen how to interpret the ECG reports taken in anterior, inferior, and posterior heart attacks in Article-F in this blog. In this article we are to study how to read the ECG reports in various conditions that may results in heart attacks other than the conditions already described. Heart attack can result from any pathological condition of the myocardium-(heart muscle.)
 |
| Fig-1A |
 |
| Fig-1B |
 |
| Fig-1C |
Check and compare the above ECG report shown in Fig-1C with the images shown in Fig-1A and 1B.
In Fig 1A a normal sinus rhythm has been drawn by hand. In Fig 1B another simulated ECG image has been drawn to demonstrate its deviations from the normal rhythm due to heart attack. It is clear from the Fig-1B that the abnormal rhythm contains an elevated and depressed ST segment.
The ST segment represents the time taken and the work done during ventricular relaxation. But the deviation indicates that the ventricles are not properly relaxed.
The elevation confirms the prediction of the immediate event of a heart attack while the depression indicates the presence of ischemic angina which may or may not result in a heart attack immediately.
Now we can interpret the model ECG report shown in Fig-1C. First check the records of the master lead -II which is the important lead that views the heart from the normal axis.
See the deviations marked in small red circles. The ST segment is elevated.
Now we can Check the unipolar electrodes aVL and aVF which also view the heart from left top and bottom respectively. They are also showing the elevation.
The elevation is more clear in the chest leads such as V4, V5, and V6 which view the heart very closely and from the left.
And hence this ECG is foretelling about the event of a severe heart attack.
In Fig 1A a normal sinus rhythm has been drawn by hand. In Fig 1B another simulated ECG image has been drawn to demonstrate its deviations from the normal rhythm due to heart attack. It is clear from the Fig-1B that the abnormal rhythm contains an elevated and depressed ST segment.
The ST segment represents the time taken and the work done during ventricular relaxation. But the deviation indicates that the ventricles are not properly relaxed.
The elevation confirms the prediction of the immediate event of a heart attack while the depression indicates the presence of ischemic angina which may or may not result in a heart attack immediately.
Now we can interpret the model ECG report shown in Fig-1C. First check the records of the master lead -II which is the important lead that views the heart from the normal axis.
See the deviations marked in small red circles. The ST segment is elevated.
Now we can Check the unipolar electrodes aVL and aVF which also view the heart from left top and bottom respectively. They are also showing the elevation.
The elevation is more clear in the chest leads such as V4, V5, and V6 which view the heart very closely and from the left.
And hence this ECG is foretelling about the event of a severe heart attack.
1.HEART ATTACK WITH BUNDLE BLOCKS: -A- RIGHT BUNDLE BRANCH BLOCK (RBBB):-
First we must know about what is the bundle and its branches, diagrammatically.

In the above diagram it is clearly seen that the electrical current which is conducted from the AV node to the Bundle of His is blocked in the right branch and passed through the left branch and arrived at the RV indirectly from the left. This is RBBB in which the right ventricle cannot receive electrical current from the HIS bundle branch but receiving it from the left ventricular muscle as shown in the diagram above.
In a similar manner the LBBB can also be understood.
RBBB and LBBB are asymptomatic and may not be serious if they are benign. But they become serious if they are with other problems in the heart such as ischemia, arrhythmias, or drug overdoses like BP medicines or antiarrhythmic medicines like beta-blockers and digoxin, etc.
In aged conditions when the heart muscles are weak these benign conditions may become violent.

Fig-2A

Fig-2B
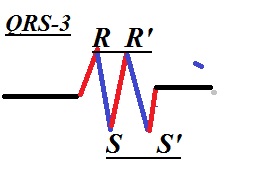
In Fig-2A there are simulated ECG drawings that have been shown to demonstrate the appearance of the rhythm in lead-II,leads-V1, and V6.
See the M shaped rhythm in lead V1 and N shaped rhythm in lead V6.
In V1 and aVR which view the heart from the right the rhythm contains one r, and one R-waves and an S-wave and no Q-wave. Hence this is an RBBB rhythm.
RBBB is many times may not be a serious problem but if it is associated with a heart attack or with a weak heart muscle it can be fatal. In RBBB as we already described the hearts axis is slightly shifted to the right.
B-LEFT BUNDLE BRANCH BLOCK(LBBB):-

Fig 2C
Compare the above model ECG taken during LBBB in Fig-2C with the simulated hand-drawn LBBB image in Fig 2B and observe the camelback like M appearance. Hence this an LBBB rhythm.




Symptoms:-
The most common symptom is syncope (fainting) or presyncope (feelings to syncope).
Causes for Bundle Blocks
1.Beta-blockers like atenolol, metoprolol
2.Calcium canal blockers like amlodipine, nifedipine
3.antiarrhythmic drugs like digoxin
If the drugs are withdrawn in doctors' supervision bundle blocks can be corrected.
2.Calcium canal blockers like amlodipine, nifedipine
3.antiarrhythmic drugs like digoxin
If the drugs are withdrawn in doctors' supervision bundle blocks can be corrected.